

Periodically, I love to tell a story of an encounter with an international medical graduate I worked with years ago. While toiling as a ward attending at our county hospital at the start of another academic year, I had paired up with a newly arrived intern from Egypt. A jovial guy who had years of practice experience under his belt, but none here in the U.S., he came to start his training in New York.
He had reasonable clinical chops, but due to his short time in America, he lacked, shall we say, U.S. cultural competency. He did not understand the nuance of our country’s open-minded ways—and by open-minded, I don’t mean the red versus blue type.
The vignette of our patient seemed simple: a middle-aged female with cellulitis of the lower extremity. We discussed the case before entering the room, and I told my charge to go to it with me at his side. He began to ask questions, but as time progressed, he started to wear an uneasy smile.
You see, the patient in front of us looked like a female. In fact, she had begun hormonal shots and had had the appropriate waist up surgery to initiate her transformation to a new gender. A big leap, our international newbie gazed into to the transgender world for the first time.
Above the blanket, everything appeared hunky dory. However, she had not acquired enough funds to finish the endeavor south of the border. You could not mistake the genotypic configuration of our patient. I forgave the phenotypic lapse. 🙂
The look on my interns face was precious. Watching him struggle made me a bit uncomfortable, but after some time, he settled in and finished the exam with minimal equivocation. His quivering lip after we finished up outside the room signaled utter bewilderment, as if to say, “we ain’t in Kansas anymore.”
After a moment, with a smile on his face, he said to me in his accented English, “ahhhhh…..Dr. Flansbaum, in my country, you don’t want to know what happens to people like that.” He just burst out laughing. You had to be there to appreciate the moment.
His innocence cracked me up, but i followed the patient encounter with an exchange on the importance of learning new culture and how he must view the true individual in front of him. He had to put aside his preconceptions drawn from earlier experiences and see the world through a new lens. I still tell the story today.
As taxing as the episode might have been, I found the whole scene priceless. Watching an international graduate take his first step assimilating into a new professional role, American style, opened my eyes once again to the valuable guidance we provide as teachers. I consider moments with them as prized as the interactions with my patients. What is the difference really? In both instances, you bestow the knowledge and comfort the other side lacks.
The learning is a two way street however, and I get as much as I receive. Over the years, I have absorbed distant perspectives on religion, the roles of gender and family in the home, and viewpoints on sickness and death. As a result, I believe my connection with trainees from other countries has made me a better person.
I say those words confidently, especially given my experience with friends and family in other fields. Because they meet too many folks like themselves, a very homogenous bunch they are, they have a limited worldview.
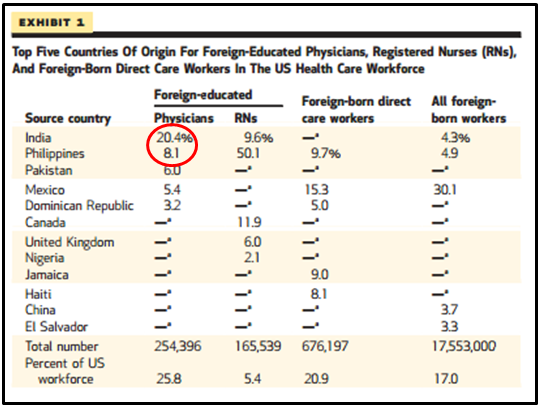
With that in mind, I found a new release in Health Affairs, Policy Solutions To Address The Foreign-Educated And Foreign-Born Health Care Workforce In The United States, informative and the short overview enhanced my understanding of the current state of IMG affairs. What follows is a hodgepodge of interesting facts:
- –Our IMG country of origin roll comprises a large number of countries (135), but a third hail from India or the Philippines:
- –20% of IMGs are American
- –IMGs are more likely to work in internal medicine or primary care and are less likely to be board certified.
- –IMGs are also more likely to work in solo practice and earn a greater percentage of their income from treating Medicaid and Medicare patients.
- –There are four major categories of visas allowing legal admission to the United States:
- 1. Family-sponsored (65%)
- 2. *Employment or education-based (15%)
- 3. Humanitarian/asylum (16%)
- 4. Diversity (4%)
- *The work visas, and you know them by name but can’t define them I am sure, include:
- –The J-1 visa: designed to facilitate opportunities for cultural and educational exchange between the United States and other nations.
- –The H-1B visa: which allows US employers to temporarily employ foreign workers in specialty occupations and are temporary and not intended to provide a path to legal permanent residency.
- –About 70–75 percent of foreign-born physicians are estimated to remain in the United States following the completion of their residency training.
- –Approximately 72 % of the IMGs who were matched to GME positions between 2008 and 2012 entered primary care fields. They will soon comprise 35% of our primary care workforce. Their overweighted task: care for vulnerable, older, or poor persons living in shortage areas.
- –Once IMGs gain legal permanent residency status however, their practice locations are largely similar to those of their US-educated counterparts.
- –IMGs encounter racism and discrimination inside and out of the medical community; may have lower rates of job satisfaction; and experience higher rates of job turnover.
How migration affects their country of origin:
- –They remit hundreds of billions dollars home…
- –HOWEVER, the transplantation here drains talent and educational costs from the coffers of their native countries.
- –Based on my reading, the latter trumps the former.
Potential policy changes to ameliorate imbalance and improve QOL (most lack depth and breadth enough to solve the problem):
- -Bonding schemes (a security deposit to insure providers return home)
- -Increase the supply of workers who are U.S. legal permanent residents
- -Reimburse workers’ home countries
- -Promote and monitor ethical migration and recruitment
- -Encourage U.S. employers to improve the experience of immigrant health workers
The looming workforce shortage, particularly in primary care, will cast immigration and training policy into a brighter light. Underfunding of GME training slots exacerbates the tension. Anyone who works with international graduates has experienced the past decade’s increasing impediments: tightening immigration policy, discrimination, and a scarcity of training slots all play a role. More strain would be an understatement, and if you speak to house staff coordinators (the administrators who really “run” the programs for the physician directors), they will tell you how the IMG applicant process has changed. Describing the transformation would require another post. Regardless, the above statistics will not remain static, and I expect a different set of numbers—probably less favorable to a heterogeneous workforce in the coming years.
On a brighter note, most international graduates can compete with the best of what the U.S. can produce. Many I would trust with my family’s life, and have. They study hard, come impeccably trained (a biased sample though), and want to be here. I believe we elevate the quality of our physician workforce with their presence. Watch the looming GME funding battle though—as the tug of war has as much to do with U.S., as it does international graduate policy.
For me, I will advocate for their presence, slots and demand permitting. They make my life richer and practice more exciting. And after all, who else would have turned me on to chicken vindaloo and biryani.
Brad,
A precious vignette with a blog that highlights the universal issues of cultural sensitivity and the moral responsibility of brain drain. I agree philosophically on the need to return trained health care providers to their country of origin (at least for some time period), but am less comfortable imposing those decisions on the individual physicians with whom I have had contact. I also wonder whether my willingness to keep software engineers and other scientists in our country is hypocritical, given the linkages between economic progress and health.
But most telling is the issue of cultural sensitivity. The cross-cultural education works both ways, and it’s nice when our colleagues and patients make the world a smaller place.
[…] about President Obama’s” end run “around the house Republicans, asks Maggie Mahar about” the catch. “ That is, in the context of proposal would support must inform their customers about missing the […]
For clinicians interested in learning more about how to provide equitable and respectful care to transgender patients, SHM would like to refer you to two resources.
The first is from Human Rights Campaign and it’s called The Healthcare Equality Index. It’s a resource for healthcare organizations on how to provide LGBT patient-centered care. http://www.hrc.org/files/assets/resources/HEI_2013_final.pdf
The second resource is a website called Out for Health, which is Planned Parenthood’s LGBT health and wellness project that provides education and information to LGBT patients and their healthcare providers. Informationfor providers can be found here: http://outforhealth.org/for-providers.html.
http://outforhealth.org/for-providers.html
[…] Posted at The Hospital Leader on […]
Thank you Meghan for your contribution regarding LGBT care. I was surprised at the blog encouraging an open mind and respect for International Graduates yet portraying disrespect for Transgender patients as endearing.
Hi Kelley
Let me clarify. No disrespect intended, and the encounter my resident had with our patient stemmed from lack of cultural competence. Any mirth stemming from the incident, I assure you, had 100% to do with an iMG immersing himself into our ways, and nothing to do with the patient’s lifestyle, appearance, or gender choice.
The interchange serves as an acute example of how someone unfamiliar with our beliefs can find themselves disconnected from the role they need to serve. The disconnection requires guidance and teaching on our part. We who serve as faculty supervisors must meet those goals.
I wish to thank and wholeheartedly endorse Meghan’s contribution.
Brad