


I have hit this topic before-copying and pasting notes—about a year ago. Let’s revisit.
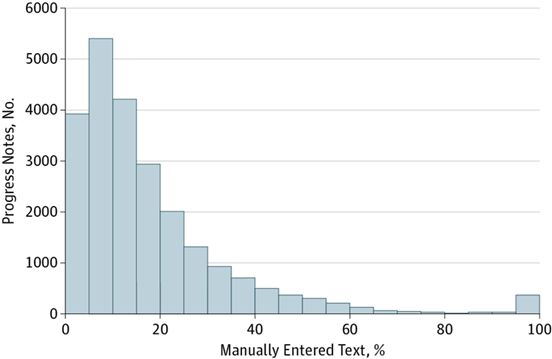
First, note the figure below. To the far right of the x-axis, you see the number of notes with > 60% + of manual entries, i.e., not pasted, in a large sample of studied notes—this from a JAMA study out of UCSF. Miniscule.
To translate the top-line finding: only 18% of text in inpatient notes are original. The rest providers pulled from other places. Sobering, but I don’t think anyone would be shocked.
Another interesting factoid:
Physicians in the U.S. write patient notes that are nearly four times longer, on average, than those in other countries. (Reason: *Billing and Regulation*)
Other issues contributing to the EMR mischief—many of which we know well:
- Copying-and-pasting content into a patient note from another source, such as a previous clinical note
- Relying on templates to prompt the user when to input relevant patient information
- Depending on auto-population tools to enter necessary patient information into data fields
- Relying on “favorites” lists to identify a patient’s medical problem, rather than searching for the most accurate or specific diagnosis
- Working outside the EHR, such as handwriting notes or communicating patient information with other providers via email
And another recent study that stuck in the back of my mind: Concordance Between Electronic Clinical Documentation and Physicians’ Observed Behavior:
Key Points
Question: How closely does documentation in electronic health records match the review of systems and physical examination performed by emergency physicians?
Findings: In this case series of 9 licensed emergency physician trainees and 12 observers of 180 patient encounters, 38.5% of the review of systems groups and 53.2% of the physical examination systems documented in the electronic health record were corroborated by direct audiovisual or reviewed audio observation.
Meaning: These findings raise the possibility that some physician documentation may not accurately represent actions taken, but further research is needed to assess this in more detail.
The bottom line here is much of the data in the H&P is pro forma and unhelpful in gleaning reliable intel on any patient encounter.
Yes, the usual caveats apply in all of the above—there will be hospital to hospital variation—but let’s not kid ourselves. I’d say this is representative of real-world affairs.
“Physicians use workarounds like copy-and-paste to make their day more efficient, said Dr. Melinda Ashton, chief quality officer of Hawaii Pacific Health. “You can discourage all you like,” she said. “If the tools don’t make it easy to do the right thing the right way, workarounds are going to occur.”
So to address EHR workarounds, she said what health systems really need to address is documentation burden.”
Progress comes slowly and changing deeply held patterns and habits are neither fast nor easy. But the scientific arc of the universe ultimately bends toward truth. I think.
Discuss amongst yourselves.
Clinician should edit . Copy and paste is a luxury for proficiency. In Documentation , integrity is vital.
The day I can’t copy, paste and edit progress notes is the day I quit. Period. We’ve got big problems in medicine, not the least of which are a mass of uninsured people, prescription drug costs, a burgeoning aged population with no plan for how to adequately care for them. I’m doing my job to the best of my ability. Don’t make it more difficult than it already is.
To start, yes, we often abuse copy paste to get the job done and often miss edits which should have been updated. True.
(And I am jealous of whomever thought of this research … fantastic and rich with info I’m sure!)
But, I feel the problem really is the documentation required for billing. Thank you copy paste for filling this need.
Ideally, the job of the note is to document key changes and interventions to pass on to other providers. Including vitals, labs, and imaging which are available in the EMR is redundant. Auto filling them into a chart doesn’t prove we’ve reviewed them.
Adding anything more than abnormal exam findings doesn’t add much value.
What I read is, we only really need 18% of the note.
The onus of changing copy and pasting should be on the system and process not on the individual.
Why does it not happen in the NHS or the rest of modern Europe
Documentation is driven by a process that is changeable and should be patient client customer centered
some hospital will not allow copy and paste I agree copy and paste is liability but EMR itself forwards notes