


A couple of months ago, I wrote about some key findings from a 2018 survey of US physicians by The Physicians Foundation. It’s no surprise to anyone working in healthcare today that the survey found alarming levels of professional dissatisfaction, burnout, and pessimism about the future of medicine among respondent physicians. Sadly, it appears that much of that pessimism is directed toward hospitals and their leaders: 46% of survey respondents viewed the relationships between physicians and hospitals as somewhat or mostly negative and adversarial.
Several physicians posted comments online, and they deeply saddened me. My heart hurt for those doctors who wrote, “I loved medicine. It was good for my soul, but medicine left me. Doctors gave up most of their power and large corporations without an ethical foundation and no god, but money took over.” Or “They are waiting so all the senior physician will retire. Nurses will become leaders who will follow administration’s lead and control physicians. Money and cost cutting is the major driver. Physicians are not valuable anymore because they have different opinions which cost a lot. There is a lot of window dressing, but they actually don’t care. They just want to run a business.” I also read “I was tossed out like dirty laundry water at age 59.” And “On a personal basis, I will try to reason with management exactly once before I bail.” Sigh.
These commenters are well-meaning physicians who had bad experiences with hospital leaders they saw as uncaring and unresponsive to their concerns as clinicians. Their experiences left them demoralized and embittered. I’m truly sorry for that.
I’m a recovering hospital administrator myself. My business partner Dr. John Nelson likes to tell people that he has successfully deprogrammed me from the way most administrators think about doctors, but he’s mostly joking (at least I think he is). I can tell you that most of the hospital leaders I have met – both when I was still an administrator and now in my consulting work – are well-intentioned people who care deeply about patients and their fellow healthcare professionals and are trying hard to do the right thing. Many of them could have earned more and had better career opportunities doing similar work in a field other than healthcare but chose healthcare out of a sincere desire to do good and help people.
A big part of the problem is that doctors and administrators come to healthcare from very different starting points, and so have very different perspectives. They generally function in separate silos, each paying attention to their own comfortable little part of that monster we call a healthcare delivery system. Often, neither administrators nor doctors have made enough effort to cross over and understand the issues and perspectives of people in other silos. As a result, it’s easy for assumptions and biases to creep in and poison our interactions.
When interpreting the behavior of others, we humans tend to overemphasize dispositional factors such as personality or motives, and to discount situational factors such as external stressors. Psychologists call this the fundamental attribution error or correspondence bias, and the result is usually heightened conflict as a result of presumed negative intentions on the part of others (“all she cares about is making a profit”) and discounting circumstantial factors that might be influencing others’ behavior (“she is facing reduced market share and a funding shortfall, and is fearful for the future of the institution”).
Add in another phenomenon known as the actor-observer bias, where we tend to attribute others’ behavior to their dispositions but attribute our own behavior to the circumstances (“that administrator lost his temper because he’s a demanding jerk, but I only lost my temper because he pushed me over the edge”).
Is it possible that hospital leaders and doctors are reading each other inaccurately, and making assumptions about each other’s intentions that get in the way of having constructive dialogue? How can we get to a place of greater trust? I don’t know the whole answer, of course, but I have a few ideas to offer.
- Intent vs. Impact
We tend to focus on the impact on us of what another person does, and to draw (sometimes incorrect) conclusions about their intentions. Consider asking yourself, “Is it the impact (i.e., the outcome) of the other person’s behavior that is bothering me so much, or is it what I believe about the other person’s intentions? This can help us become more aware of and introspective about our own assumptions and biases, and potentially to dig deeper into understanding the other person’s intentions before making a judgment.
- Walk in Each Other’s Shoes
Working in our own silos creates isolation rather than engagement. I have some regrets about my time as a hospital administrator – things I wish I had done differently or better. At the top of that list is my regret that I didn’t spend more time in clinical areas, talking with clinicians and patients and understanding what really goes on in the parts of the hospital where care is delivered. I wish a few doctors had invited me to round with them or to gown up for a surgery. I also regret that I didn’t invite doctors to “round” with me and enter my hospital administration world to better understand the business pressures I faced. I encourage you to (respectfully) invite that irritating administrator to come spend a few hours rounding with you and experiencing the world from your perspective. And even consider asking if you can come shadow them for several hours one day, just to learn more about their world and the challenges they face.
- Build Social Relationships
When you build social relationships with others, be they hospital leaders or the orthopedic surgeons you have tense relationships with, you make it harder for both them and you to dismiss each other’s perspectives, issues, and concerns. So I encourage you to look for opportunities to build social connections with hospital leaders outside of work and find things you have in common. Invite an administrator and her spouse to dinner at your home. Invite your C-suite to join your group at happy hour at the local brewpub. Participate in (or help organize) a hospital-wide softball team, music appreciation group, book club, or podcast lovers’ interest group.
- Educate Yourself
Physicians don’t learn a lot about the financial underpinnings of healthcare delivery in medical school or residency; in fact, most of them don’t even understand how to select a CPT code upon entering practice. Experts on physician-administrator relationships recommend that physicians invest in educating themselves about healthcare policy and finances, and about the market realities of their current practice setting. You can seek insight from leaders in your institution, take classes at a local or online college or university, or even pursue a master’s degree in healthcare administration or finance. Similarly, you could engage hospital leaders in a process to teach them more about clinical medicine and help them learn first-hand your language and your perspective.
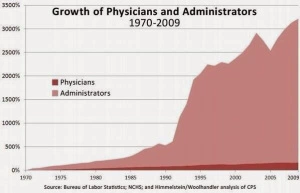 The presence and influence of healthcare administrators isn’t going away any time soon; in fact, the number of administrators in healthcare is growing at a much faster pace than the number of physicians (see chart). So it is in your interest to build a better relationship with the hospital leaders who are positioned to wield influence over your clinical practice, rather than just dismissing them or letting their (often inadvertent or ill-informed) actions contribute to your professional dissatisfaction and burnout. There is some good news on the horizon: increasingly these administrators are your former hospitalist colleagues. And one day soon you may find that the administrator influencing how physicians practice in your institution is you!
The presence and influence of healthcare administrators isn’t going away any time soon; in fact, the number of administrators in healthcare is growing at a much faster pace than the number of physicians (see chart). So it is in your interest to build a better relationship with the hospital leaders who are positioned to wield influence over your clinical practice, rather than just dismissing them or letting their (often inadvertent or ill-informed) actions contribute to your professional dissatisfaction and burnout. There is some good news on the horizon: increasingly these administrators are your former hospitalist colleagues. And one day soon you may find that the administrator influencing how physicians practice in your institution is you!
Leslie-
Good blog post. I am just wrapping up my doctoral research and there is a strong thread that resonates with your topic here. One of the implication of my study is more collaboration (e.g., conversation) with hospital leaders, hospitalist group leaders and hospitalists. One trend that has continues and impacts hospitalists are continued vertical integration. Vertical integrations that reduce access for hospitalists to talk directly with hospital decision makers has also influenced the disconnect among people.
dea
Dea Robinson
Doctoral Candidate
Colorado State University
Leslie,
Well done! As a hospitalist who has “gone to the dark side” as a dyad partner with administration, your article is timely and necessary reading for all. I spend the great majority of my time facilitating communication between exceptionally committed and highly skilled team members. You have elegantly reflected many of the reasons for distrust and misalignment between providers and administrators. It is truly a shame that the relationship is seen as adversarial or “win lose” as that mentality holds back collaboration that is essential for our patients in the current landscape. The teams that are best able to leverage collaboration from these two essential components of hospital medicine will be those teams whose patients benefit the most. Again, my appreciation for your perspective and willingness to challenge the current stereotypes.
No offense but this comes off as well meaning but naive. In many doctors’ experience the administration doesn’t want understanding or input, they want obedience. When policy changes without explanation, they want obedience again.
Leslie-
I love the idea of walking in each other’s shoes. However, I think that this article falls a bit flat given the current rift between admin and clinicians. I think that it may be a good idea to do a follow up article co-written with a physician colleague (who is still practicing clinically and not only involved in admin) to provide both perspectives.
Additionally, I disagree that the burden should be on physicians to seek out ways to learn about financial aspects of healthcare. There are very few clinicians who have the time to obtain a masters in health administration, for example. The fact that clinicians know so little about healthcare policy and business is a current failure of our medical education and would be best incorporated into our medical training, residency training and, most importantly, when we start our new position out of residency. We need directed education on this subject as a self directed strategy is likely to result in inefficient and insufficient acquisition of knowledge.
Laura Nichols, MD
Sanford Health